Kidney Cancer
Kidney cancer is primarily a surgical and chemotherapy disease. Radiation is reserved for palliation, for the most part. Renal cell carcinoma and clear cell carcinomas of the kidney have been thought to be largely radio-resistant, but experience has shown otherwise. With higher doses/fraction, excellent palliation has been obtained in treating metastatic kidney cancers. It is likely that the α/β ratio is lower than other cancers with a broad shoulder of the linear quadratic curve.
Anatomy
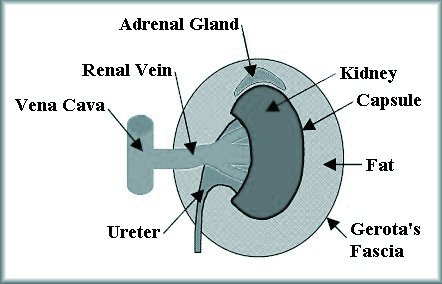
The anatomy of the kidney consists of the renal cortex which is surrounded by the renal capsule. The adrenal gland sits on top of kidney and is embedded in the perirenal fat. The complex is surrounded by Gerota's Fascia.
From outer to innermost layers:
- Gerota's fascia surrounds all
- Perirenal fat is deep to Gerota's facia and includes the adrenal gland, also deep to Gerota's fascia
- Adrenal gland is embedded in the peri-renal fat
- Kidney capsule
- Renal cortex
Demographics and Natural History
Therae are about 51,000 new cases of renal cancer each year in the US. The incidence of RCC has been rising by about 2%/year over the last 30 years (SEER). Men are more commonly diagnosed with RCC than women. Renal cell carcinoma is commonly diagnosed in the 7th decade. Renal cell tumors account for 6% of all urinary tract tumors. Approximately 10% will present with a palpable abdominal mass.3% will have bilateral disease at diagnosis.
The "classic triad" of symptoms include hematuria, flank pain and a palpable mass. Signs of fever, night sweats and weight loss suggest the presence of metastatic disease. Although many do not screen for bladder cancer in RCC, the relative risk of bladder cancer is 1.5, with suspicion that this increased risk is associated with smoking.
Paraneoplastic syndromes occur in20% of all patients. Several paraneoplastic syndromes are seen in RCC:
- hypercalcemia
- hepatic impairment
- hypertension
Natives of the Balkans have a 50 - 100 fold increased incidence of renal cell carcinoma. Theoretically, this may be related to the high levels of nephropathy from heavy metal exposure. If data were available, one would expect to see similar distributions in the other former Soviet States.
Genetic Factors are associated with a variety of syndromes. Up to 4% of RCC are familial. These syndromes include:
- Von Hippel-Lindau Syndrome (autosomal dominent -- hemangioblastomas, pheochromocytoma, RCC, renal angioma)
- Birt-Hogg-Dube syndrome
- Tuberous Sclerosis
- Hereditary papillary RCC
- HRCC (met proto-oncogene)
- Familial leiomyomatosis
- RCC (fumarate hydratase)
- Familial clear cell RCC
Sporadic RCC is characterized by a mutation in the VHL tumor suppressor gene on chromosome 3p25. This tumor suppressor gene is silenced in > 25% of sporadic RCC.
Modes of Spread, Metastatic Sites and Recurrence
Renal cell cancer commonly metastastasizes and recurs in the Lung (1), bone (2) and regional lymph nodes. The signficant prognostic factors are: TNM staging, performance status and Furhman Grade.
Recurrence generally occurs between years 3 and 5 after nephrectomy. Follow up imaging consisting of chest xray or CT of the chest and CT or MRI of the abdomen should be peformed. Recurrence can occur even after 5 years and RCC patients should be followed for life. Sporadic reoccurrences have been found even 40 years down the road.
Pathology
Pathologic subtypes of RCC:
- Clear Cell
- Chromophilic
- Chromophobic
- Collecting Duct
Clear cell cancer of the kidney is the most common renal cell carcinoma. These demonstrate large cear cells with abundant cytoplasm. RCC is graded on the Fuhrman grading system from 1 - 4 based on nuclear roundness, size, nucleoli presence and clumped chromatin.
Workup and Staging
Renal cell carcinoma requires a tissue diagnosis. Often nephrectomy is both diagnostic and therapeutic. Percutaneous biopsy can be used in medically un-fit patients. Of the biopsied specimens, 33% of small tumors are benign.
Imaging Work up
Imaging workup includes contrast enhanced CT or MRI of the abdomen and chest imaging. Consider bone scan and MRI of the brain if clinically indicated.
Staging
| T1a | Limited to kidney and ≤ 4 cm |
| T1b | Limited to kidney 4 - 7 cm |
| T2a | > 7 cm and limited to kidney |
| T2b | > 10 cm and limited to kidney |
| T3a | Grossly invades renal vein or its segmental branches or extends into perirenal and/or renal sinus fat but not beyond Gerota's fascia |
| T3b | extends into the vena cava below the diaphragm |
| T3c | Extends into the vnea caava above the diaphragm or invades into the wall of the vena cava |
| T4 | invades beyond Gerota's fascia |
| T Stage | N0 | N1 | M1 |
| T1 | I | III | IV |
| T2 | II | III | IV |
| T3 | III | III | IV |
| T4 | IV | IV | IV |
There are other RCC staging systems that are widely used. They include
- Robson modification system
- Flocks and Kedsky system
- Jewel Strong Classification
Treatment
The treatment of renal cell cancer is primarily surgical and chemotherapy. For locally confined renal cell carcinomas, there are a number of surgical options, but the most common is nephrectomy.
- Open nephrectomy
- Laparascopic nephrectomy
- Pertutaneous CT guided cryoablation
- Partial Nephrectomy
There have been retrospective studies examining open nephrectomy compared with laparascopic nephrectomy. There was no difference in disease free survival found in these studies. (2009). For patients with bilateral RCC, nephrectomy remains the primary treatment, if the lesion is small. A nephron sparing nephrectomy can be attempted.
There are a number of chemotherapeutic agents and immunotherapy agents tested in renal cell carcinoma. Not all are effective.
IFN-α-2b has been examined in a prospective randomized study and shown to be ineffective with no EFS or OS benefit in patients with post surgical relapse. (2003).
For patients with metastic disease, the first line treatments are:
- Surgical cytoreductive nephrectomy
- Metastatectomy for oligometastases
- Sunitinib
- Temsirolimus
- Bevacizumab and IFN
- high dose IL-2
- sorafenib
For clear cell varients cytotoxic chemotherapy may be considered.
Sorafenib inhibits multiple kinase pathways including the following:
- Raf kinase
- PDGE
- VEGF
- c-KIT
- RET
- CSF1R
- flt3
Sunitinib also inhibits similar kinase pathways.
Palliative nephrectomy is useful in controlling local signs and symptoms of pain related to the primary tumor.
Metastatic resection in oligometastases suggests (from retrospective study -- Kavolius 1998) curative resection in patients with metastatic lesions in renal cell cancer improves survival compared with sub total resection of patients or those with noncurative salvage attempts. Kavolius found 44% (curative) 14% (sub total resection) and 11% (non-curative salvage) improvements in overall survival. This evidence is the basis for re-operation.
Radiation Therapy
Radiation therapy is primarily reserved for palliation. RCC has a broad shoulder of the linear quadratic curve and is not radio-insensitive as was previously thought. Because of its radiobiologic characteristics, treatment may be improved with higher doses per fraction to a lower overall dose. Stinauer at the University of Colorado (2011) published a report on stereotactic body radiosurgery in 13 patients treated for metastatic RCC. She stereotactic body radiotherapy and converted doses delivered to an equivalent "single fraction equivalent dose" or SFED. Patients were treated to 40 - 50 Gy in five fractions (8 - 10 Gy / fraction) or 42- 60 Gy in 3 fractions (14 - 20 Gy/fraction). The local control rate at 24 months was 100% for SFED ≥ 45 Gy v. 54% for SFED < 45 Gy.